Healthcare Marketing is No Longer “Consumer vs. Referral” - It’s Both
Healthcare marketing strategy is often framed as a binary choice: consumer-driven or referral-driven.
That framing is increasingly outdated and strategically risky.
In the most recent Results Roundtable, healthcare marketing and strategy leaders gathered to discuss Deloitte’s article, The Dawn of a New Health CEO, which positions the consumer as the “CEO of their health journey.” The article provided a useful starting point, but the discussion quickly moved beyond a simple consumer empowerment narrative.
One theme surfaced repeatedly: decision ownership in healthcare does not sit at one extreme or the other. It exists along a continuum shaped by acuity, urgency, trust, financial exposure, and operational friction.
Oversimplifying that reality can distort investment decisions, silo teams, and create blind spots in growth strategy.
The Decision Ownership Continuum
Consumers have more information, digital tools, transparency, and agency than ever before. That much is clear.
But empowerment is not universal.
Decision ownership varies significantly depending on:
Acuity and complexity
Emotional intensity
Caregiver involvement
Financial exposure
Physician influence
Time sensitivity
A practical way to evaluate this dynamic is through a continuum.
A practical way to evaluate this dynamic is to view decision ownership along a continuum from consumer-led to referral-driven care.
Healthcare Decision Ownership: Consumer-Led to Referral-Driven
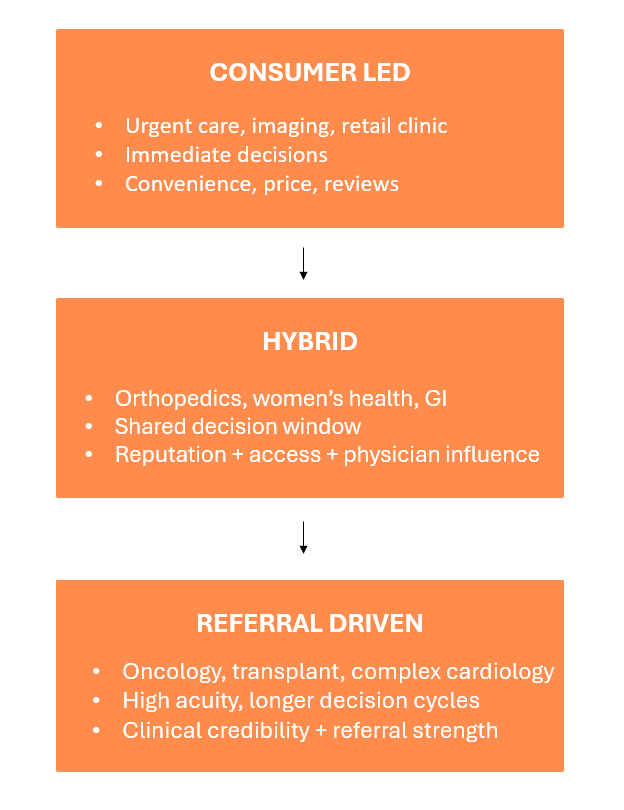
Low-acuity services such as urgent care, retail clinics, imaging, and cosmetic dermatology tend to be consumer-led. Speed, convenience, reviews, and price transparency dominate.
High-acuity specialties such as oncology, transplant, and complex cardiology remain heavily referral-driven. Clinical expertise, outcomes, and physician trust anchor the decision.
Between those poles sits a large and growing hybrid category. Orthopedics, women’s health, GI, and behavioral health often involve shared decision-making between physician and patient.
The critical insight is that most service lines now operate in hybrid territory.
Even in traditionally referral-driven specialties, patients increasingly verify provider credentials, research outcomes, read reviews, seek second opinions, and ask for specific specialists by name.
Referral-driven no longer means consumer-passive.
The Organizational Misalignment Problem
As decision behavior becomes more hybrid, organizational design has not always kept pace.
Most health systems still separate:
Consumer marketing and digital acquisition
Physician relations and referral development
Operations and access teams
Each operates with distinct KPIs, budgets, and reporting structures.
Consumer acquisition is optimized around measurable conversions such as cost per appointment or digital attribution. Referral growth is measured through relationship depth, referral volume, and downstream revenue — metrics that are often less visible in traditional marketing dashboards.
This creates predictable distortions.
Consumer-direct services may receive disproportionate media investment because ROI is easier to quantify. Referral-dependent specialties that drive significant margin often rely on longer conversion pathways that appear less visible in performance reports.
Budget allocation begins to reflect internal structure rather than real-world decision behavior.
When teams optimize independently, strategy fragments, even though patients experience the system as a single journey.
Hybridization Is the New Normal
One of the clearest themes from the discussion was the continued expansion of hybrid behavior.
Patients validate referrals online. They compare institutions. They leverage AI tools for research. They request specific providers. Physicians increasingly report encountering more informed and opinionated patients.
Influence now accumulates from multiple sources before a specialist appointment ever occurs.
Treating consumer marketing and referral marketing as separate lanes misses the reality of how decisions are actually shaped.
Friction Reduction Is a Growth Strategy
Another recurring theme was ease.
In many service lines, the differentiator is not brand awareness. It is friction reduction.
Scheduling specialist appointments at the point of referral. Seamless care coordination. Transparent access lines. Reduced administrative complexity.
Patients may accept a physician’s recommendation, but if scheduling is slow or confusing, they pivot.
Operational design has become marketing leverage.
For consumer-led services, friction reduction may mean online scheduling and price transparency. For hybrid services, it requires coordinated referral navigation and reputation management. For referral-driven specialties, access efficiency and specialist availability often matter more than incremental awareness spend.
In a margin-constrained environment, eliminating operational bottlenecks often produces more growth impact than increasing media investment.
From Binary Thinking to Strategic Alignment
The consumer versus referral framing is too simplistic for today’s healthcare landscape.
Decision ownership is contextual.
Hybrid behavior is expanding.
Operational friction influences growth as much as brand awareness.
Marketing structure must align with real-world decision pathways.
As margin pressure intensifies and expectations rise, healthcare leaders cannot afford to treat decision behavior as static or binary.
Aligning strategy with how decisions are actually made is no longer optional. It is a competitive requirement.
Interested in continuing the conversation? Connect with Tim Duer, who led the session, at tduer@causewaysolutions.com.